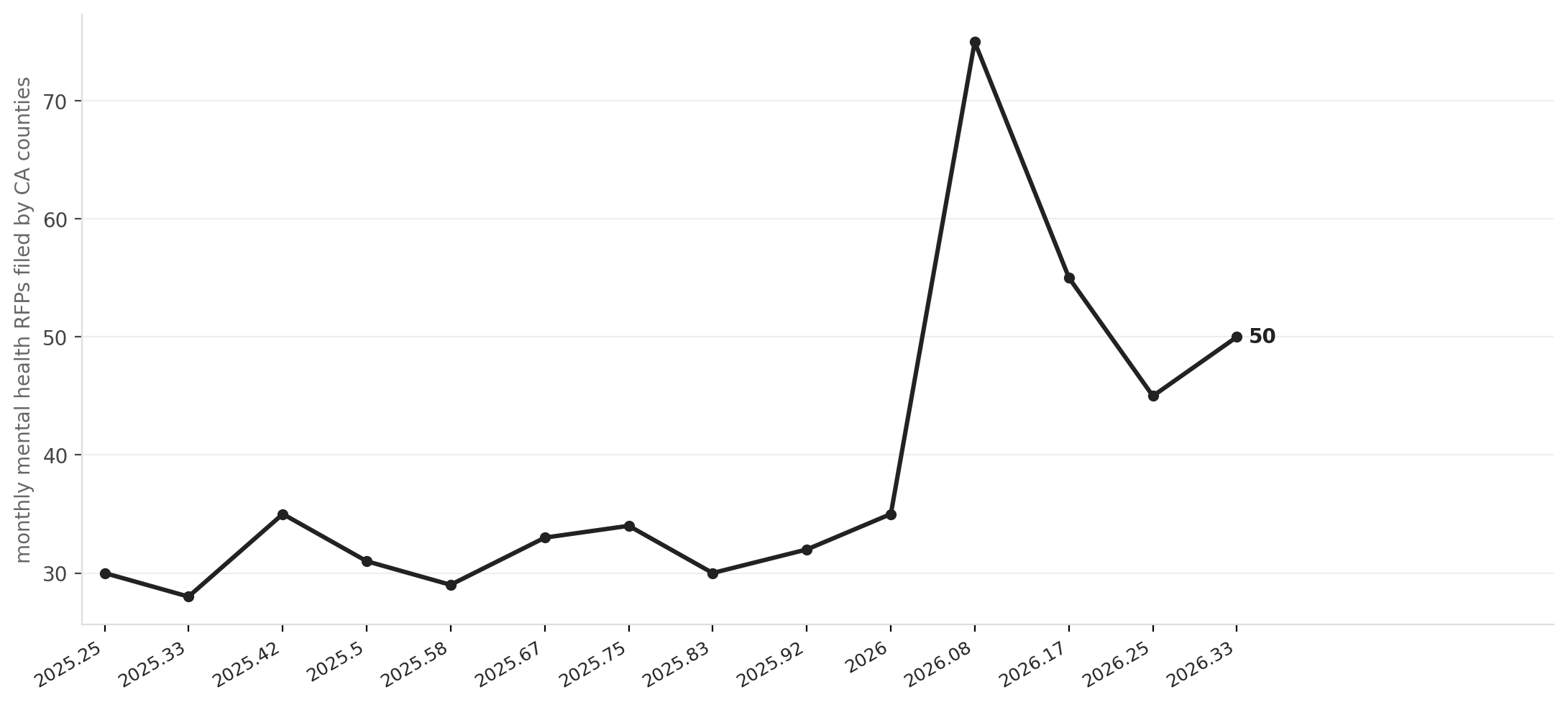
California counties issued roughly 50 mental health procurement solicitations in May 2026, nearly double the 12-month monthly average of 32, and the acceleration is not random. It is the sound of a $4.4 billion bond hitting its execution phase all at once.
Proportion 1's Behavioral Health Infrastructure Bond Act, passed by voters in March 2024, distributed $3.3 billion to 124 projects across 42 counties in May 2025. Governor Newsom announced a second round of $1.18 billion in March 2026, bringing total Prop. 1 spending to nearly $5 billion and pushing projected statewide capacity beyond the initiative's original goals: 6,919 residential treatment beds and 27,561 outpatient slots across both rounds. The sharpest single-month spike in the 14-month RFP series, 75 solicitations in February 2026, landed almost exactly when Round 2 awards were being finalized, a coincidence that is almost certainly not one.
The forcing function is a hard administrative deadline. Prop. 1 requires every California county to file an integrated behavioral health plan covering fiscal years 2026 through 2029 by June 30, 2026. That date is not a suggestion. Counties that have not converted their bond awards into active vendor contracts and service agreements by then risk losing uncommitted funds and, more immediately, failing a compliance checkpoint that determines their eligibility for future state behavioral health dollars.
Source: NationGraph.
The counties feeling that pressure most acutely are the larger urban and suburban ones now executing on Round 1 and 2 awards. San Diego County alone issued 10 mental health RFPs in the current 30-day window, spanning In-Home Outreach Teams, High Fidelity Wraparound services for youth, and Clubhouse Services parceled across six geographic lots. Sacramento County is procuring behavioral health services for youth alongside specialized equipment. Alameda and Shasta counties are also active in the current cycle. The February spike and the May plateau are both concentrated in these operationally urgent counties, not in the archival filings from smaller rural jurisdictions that account for a substantial portion of the raw RFP count.
The scale of what is being committed is worth naming plainly. DHCS Director Michelle Baass described the combined BHCIP rounds as building "capacity so families in rural, Tribal, and underserved areas can count on consistent, high-quality care for the next three decades." Three decades. Counties are signing long-term facility leases, construction contracts, and multi-year service agreements on a timeline driven by a bond deadline, and the operating assumption embedded in all of it is that California's Medicaid program remains roughly intact.
That assumption is now under pressure. Proposed federal Medicaid cuts moving through Congress are estimated to cost California between $10 billion and $20 billion annually. California runs the largest Medicaid program in the country, with nearly 15 million enrollees, and county behavioral health systems are structurally dependent on Medi-Cal reimbursements to pay the clinicians, case managers, and peer support specialists who would staff the facilities now being built. A facility that opens in 2027 with bond-funded construction but a 20 percent Medi-Cal reimbursement cut baked in is a facility counties may not be able to operate at the capacity for which it was designed.
The federal grant pipeline adds another layer of complexity. HUD has obligated $371 million to California mental health and housing-linked projects in the trailing 12 months, HHS has committed $201 million, and the Board of State and Community Corrections another $159 million. Those commitments are real and already in the procurement pipeline. But they are one-time capital infusions, not recurring operating revenue, the same structural distinction that separates building a clinic from keeping it staffed.
None of this means the procurement surge is misallocated. The gap in California's behavioral health infrastructure, particularly for residential and transitional-level care, is documented and large. The Legislature and voters decided in 2024 that closing it required a bond, and Round 1 and Round 2 awards have moved faster than most capital programs of this scale. The question counties are now navigating is whether the operating revenue model they assumed when they wrote their project applications survives the federal budget environment they are actually entering.
The June 30 deadline is six weeks out. Counties still finalizing their integrated behavioral health plans are, right now, deciding which contracts to execute and at what service volumes. The next signal to watch is whether the round of facilities breaking ground in late 2026 are staffed to capacity when they open, or whether the gap between what was built and what can be operated becomes the defining story of Prop. 1's implementation.