Arkansas issued seven mental health–related RFPs in the trailing 30 days through mid-June 2026, against a 12-month baseline of roughly two per month. That 3.5x spike is not a coincidence of timing. It is what happens when the largest single behavioral health investment in state history collides with a procurement calendar and a system that is, by at least one national assessment, at catastrophic capacity.
The money came first. In December 2025, the federal government awarded Arkansas $208,779,396 through the Rural Health Transformation Program, a fund created by H.R. 1, the legislation signed July 4, 2025, specifically to offset an estimated $155 billion in rural Medicaid spending cuts over the next decade. Arkansas applied for nearly $1 billion over five years and received $209 million for fiscal year 2026 alone. The award runs through October 2030, and as of mid-June, according to the Governor's announcement, not a dollar of it has been disbursed. On May 4, Governor Sarah Huckabee Sanders formally opened the sub-application portal at ArkansasRHTP.com. The RFP surge began almost immediately after.
The RHTP award is the dominant piece of a larger backlog. Arkansas currently holds 46 active federal mental health and behavioral health grants totaling $267 million in obligated funds. Only $28 million of that has actually moved out the door. The state is sitting on roughly $239 million in committed federal behavioral health money that has not yet reached a provider, a clinician, or a patient.
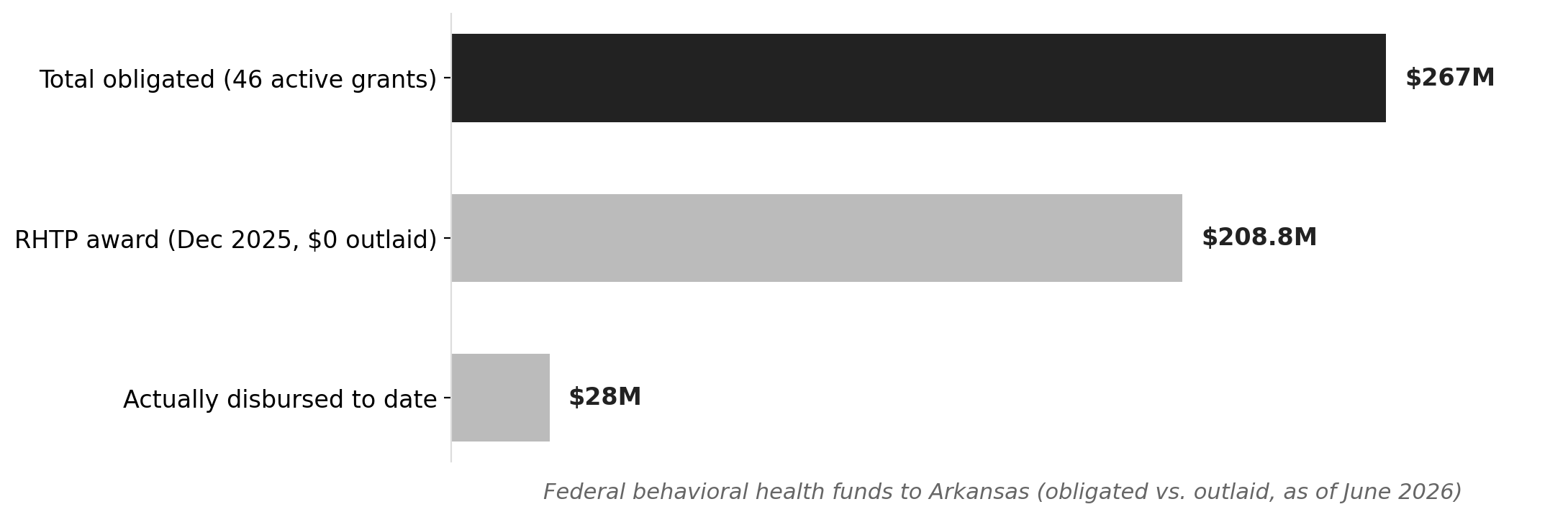
Source: NationGraph.
The procurement activity now underway reflects the urgency of closing that gap. The Arkansas Department of Human Services is soliciting behavioral health clinicians for Southeast Arkansas through the Southeast Arkansas Human Development Corporation. The Department of Transformation and Shared Services is running RFPs for Community Mental Health Centers, with vendors including Banner and Success among those in play. The Little Rock School District posted a separate solicitation for school-based outpatient mental health services. These are not coordinated announcements from a single agency. They are independent agencies, in different parts of state government, all hitting the market in the same month.
What makes the timing more than a paperwork story is what Arkansas is actually trying to staff. Inseparable, a national behavioral health advocacy organization, identified Arkansas in March 2026 as one of only four states in the country with catastrophic shortages across all three behavioral health systems simultaneously: inpatient hospitals, community providers, and crisis care. Delaware, Iowa, and Nebraska are the others. All 75 Arkansas counties carry documented health access gaps. About 45 percent of Arkansans live in rural areas, concentrated in the Delta, the Ozarks, and the southwest, where hospital vulnerability and chronic disease rates are highest.
The workforce problem is structural, not incidental. A 2024 DHS study of community mental health centers documented a persistent cycle: clinicians complete training at CMHCs, accumulate licensure hours, and leave for private practice. The state loses the provider and keeps the shortage. The 2025 General Assembly passed Act 1022, creating a framework for a Behavioral Health Loan Forgiveness Program intended to make CMHC and rural practice financially competitive with private alternatives. The program's framework exists; the implementing rules and funding mechanisms are still being built.
Arkansas is also standing up a 24-hour behavioral health crisis call center and equipping first responders with telehealth tablets under $30 million in state funds approved in 2024, efforts that require not just technology but staffers on the other end of the line. The Arkansas Center for Health Improvement has published an overview of how RHTP dollars are meant to flow through the state's rural health system, but the program's architecture depends on providers who can actually accept and deploy those funds.
For Arkansans in underserved counties, the procurement surge is a necessary precondition, not a solution. RFPs become contracts, contracts become services, and services require clinicians who are not yet hired into jobs that are not yet funded at organizations that are not yet certified. The lag between a federal award and a patient receiving care in a Delta county can run 18 months or more under normal circumstances. Arkansas is not operating under normal circumstances: it is trying to compress that timeline while simultaneously building the workforce pipeline that would make expansion sustainable.
The next signal to watch is how many of these RFPs close with qualified vendors and at what rates. A procurement surge that produces thin response pools or failed awards would indicate the workforce shortage is already constraining the state's ability to spend what it has. The RHTP sub-application portal is open now. The governor's office has until October 2030 to show results, but the window for standing up new providers before the next federal budget cycle narrows every month the money sits unspent.