Maine posted six opioid-response procurement solicitations in the last 30 days against a trailing average of fewer than one per month, an eightfold spike driven not by a worsening crisis but by three institutional forces arriving at the same moment.
All six RFPs trace to a single source: Lewiston, Maine's second-largest city, which cycled through successive rounds of its Community Opioid Services solicitation in May 2026. That concentration matters. Lewiston is not an outlier city that stumbled into urgency on its own. It is the first municipality to work through the full loop that Maine's new accountability architecture demands, spending, documenting, and re-procuring, while most of the state's 39 local subdivisions still sit on the bulk of their allocations. By comparison, Vermont, Massachusetts, and New Hampshire posted a combined seven opioid RFPs over the same 30-day window. This is a Maine-specific event.
The proximate cause is LD 110, enacted in 2025, which imposed the state's first mandatory reporting requirement on how local governments spend opioid settlement dollars. The initial comprehensive report, presented to the Legislature's Health and Human Services Committee in early 2026, landed with political force: Maine municipalities had spent just $3 million of the $22 million they had received, less than 15 percent in roughly four years. The public criticism that followed was immediate, and the pressure to both spend and document that spending visibly accelerated procurement activity in February and March 2026, the two months before the current spike.
Source: NationGraph.
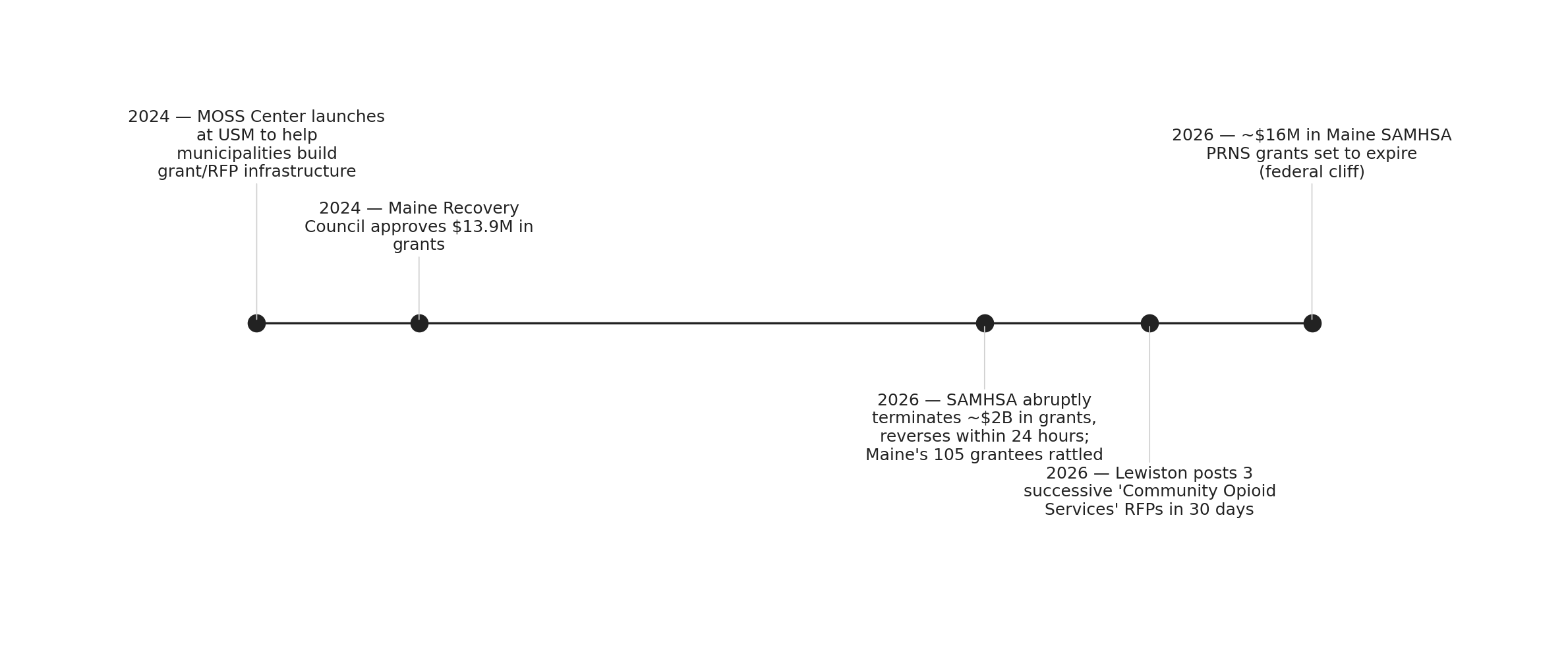
Lewiston had already been moving. The city has committed roughly half of its $1.05 million settlement allocation to crisis workers, recovery housing, sharps containers, and youth prevention programs. Its May 2026 solicitations represent the next procurement cycle, not the first. The Maine Opioid Settlement Support Center, housed at the University of Southern Maine's Cutler Institute and launched in mid-2024 specifically to help municipalities build grant and RFP infrastructure, has been the intermediary that made Lewiston's pace possible. Cities without that technical support are still building the systems Lewiston now iterates on.
The second force is federal. On January 13, 2026, SAMHSA issued termination letters for an estimated 2,800 grants totaling up to $2 billion in behavioral health funding before reversing course within 24 hours. The episode left Maine's 105 active SAMHSA grantees in what one account described as "an environment of uncertainty", and that uncertainty has not resolved. Maine DHHS holds five SAMHSA PRNS-category grants totaling roughly $16 million, all set to expire by September 2026. A separate $7.6 million substance abuse block grant expires the same month. If SAMHSA's PRNS programs are ultimately eliminated under the proposed federal budget, Maine could lose nearly $4 million in SUD treatment and recovery funding, according to estimates from the Drug Policy Alliance. The rational response for any organization that depends on that money is to lock in contracted services now, while state settlement dollars are available and the federal safety net remains technically intact.
The third force is a distribution lag catching up to reality. The Maine Recovery Council, which controls 50 percent of the state's estimated $261 million in total settlement receipts through 2038, approved $13.9 million in grants in November 2024, but all of that money flowed to recipients in 2025. Procurement to actually deploy those grants is happening now. The pipeline from settlement receipt to approved grant to contracted service has a multi-year lag built in, and 2026 is when the first full cycle of that lag completes.
For Mainers outside Lewiston, the immediate implication is asymmetric. Communities with access to intermediary support, places that engaged with the MOSS Center or already had grant-writing capacity, are moving through procurement cycles. Rural towns without that infrastructure are more likely to be in the group that has spent little or nothing from their allocation, and the political pressure created by LD 110 has not yet translated into procurement capacity for all of them.
Nationally, CDC data shows a nearly 16 percent decline in overdose deaths from December 2024 to November 2025, a meaningful improvement. But Maine's fragmented rural geography means service delivery is almost entirely procurement-dependent: providers must be contracted to reach populations in small towns that have no institutional infrastructure of their own. The RFP is not an administrative formality here. It is the mechanism by which the service exists at all.
The next signal to watch is September 2026. That is when Maine DHHS's five expiring PRNS grants and its substance abuse block grant all reach their end dates. Whether the organizations currently holding those contracts can bridge to state settlement funding, or face a gap, will depend on how quickly the remaining 38 local subdivisions move from the scrutiny of LD 110 to the procurement activity Lewiston is already running.