Minnesota counties have issued 10 mental health RFPs in the last 30 days, double the roughly five-per-month pace they held over the prior year, and the surge is concentrated where the money landed first: Dakota County has put out three solicitations, Hennepin County two, the City of Minneapolis two, and Ramsey County one. The Minnesota Department of Human Services added a statewide children's mental health screening RFP on top of that. Behind these procurement notices sits a straightforward problem: legislators appropriated the money, federal agencies released the grants, and now county contracting desks are the one chokepoint standing between policy and delivered services.
Two forces converged in mid-2026 to create the pressure. On February 2, SAMHSA distributed $794 million in block grants nationwide, including $319 million for community mental health services, the first allocation of the annual cycle. Minnesota received approximately $6 million in newly obligated Mental Health Block Grant tranches, with a spend-down clock running to September 2027. Federal grant money that isn't contracted out doesn't sit waiting; it lapses. At the same time, Minnesota's 2026 legislative session closed with a stack of new appropriations: a $200 million stabilization agreement for Hennepin County Medical Center, $11.89 million in school-linked behavioral health grants, and $3.8 million for mobile crisis teams. All of it requires county-level implementation contracts to be in place before the fiscal year turns.
The architecture of Minnesota mental health delivery makes this dynamic nearly automatic. Under the Comprehensive Adult Mental Health Act, counties route every new state or federal dollar through their human services boards before a single appointment gets scheduled. That pass-through structure means a bill signing in St. Paul or a press release from SAMHSA translates within weeks into an RFP on a county procurement portal. When funding arrives in a single compressed window, the RFP volume follows.
Source: NationGraph.
The legislative session sharpened that pressure further. SF1599, signed into law this session, eliminates cost-sharing for mobile crisis services statewide and establishes state provider standards, which means counties can no longer rely on informal arrangements, they must hold signed contracts with qualified providers. HF2213 creates a new grant program for school districts and mental health providers to co-locate services, requiring a separate procurement round. A targeted bill, HF2295/SF2943, directs crisis services funding specifically toward Dakota County, which helps explain why that single county accounts for three of the ten recent RFPs on its own.
The urgency also reflects a structural supply problem that predates this funding cycle. As of January 2026, 23 of Minnesota's 87 counties were wholly short of mental health providers, meaning demand for qualified contractors exceeds what the local market has historically supplied. Counties in the Twin Cities metro dominate the current issuance wave because they have the procurement infrastructure to move quickly, but rural provider gaps will push a subsequent contracting wave outward as school-linked and mobile crisis programs require coverage in counties that don't yet have the vendor relationships in place.
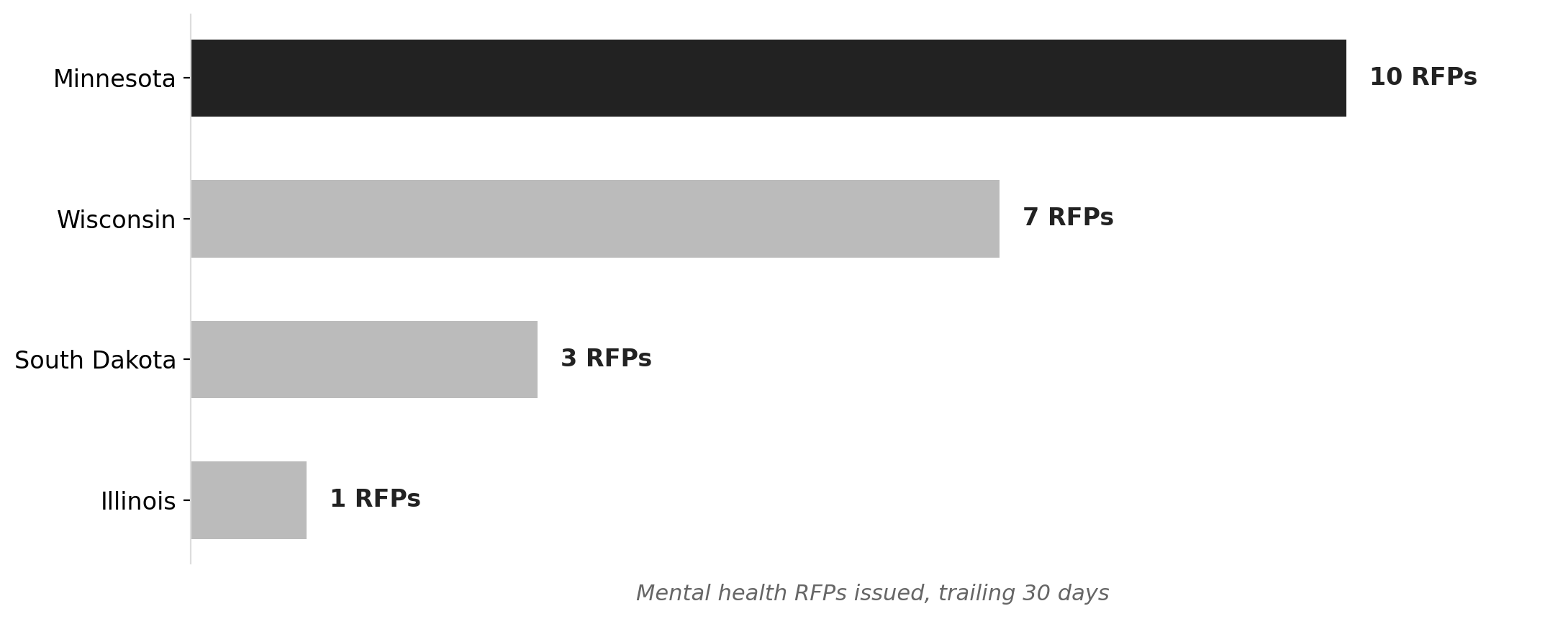
The scale of the existing federal investment makes the doubling more striking, not less. Minnesota currently holds $538 million in active federal mental health grants across 203 awards, headlined by a $193 million Rural Health Transformation grant to the Department of Health and a $22.6 million Opioid STR grant to DHS. The current RFP surge is being layered onto that infrastructure, not built from scratch. Minnesota is also outpacing its Midwest neighbors in procurement activity: ten mental health RFPs in 30 days against Wisconsin's seven, South Dakota's three, and Illinois's one.
For residents, the most visible near-term change will be in mobile crisis response. SF1599's provider standards mean that counties contracting under the new law must field teams that meet state specifications, and the $3.8 million appropriation gives them the dollars to do it. School-linked behavioral health will expand next, as HF2213 grants move through the contracting pipeline into the fall academic year.
The signal to watch is whether the provider market can absorb the demand. County procurement offices can issue RFPs at double speed; they can't conjure qualified bidders. If the rural counties with existing shortages reach their own contracting deadlines and find too few respondents, some of the new legislative dollars may not make it to patients before fiscal timelines foreclose the option.