Researchers at Emory University School of Medicine in Atlanta are pursuing something the PTSD field has struggled to achieve for decades: a way to stop the disorder from developing in the first place, using a non-invasive brain stimulation technique delivered in the critical days after trauma.
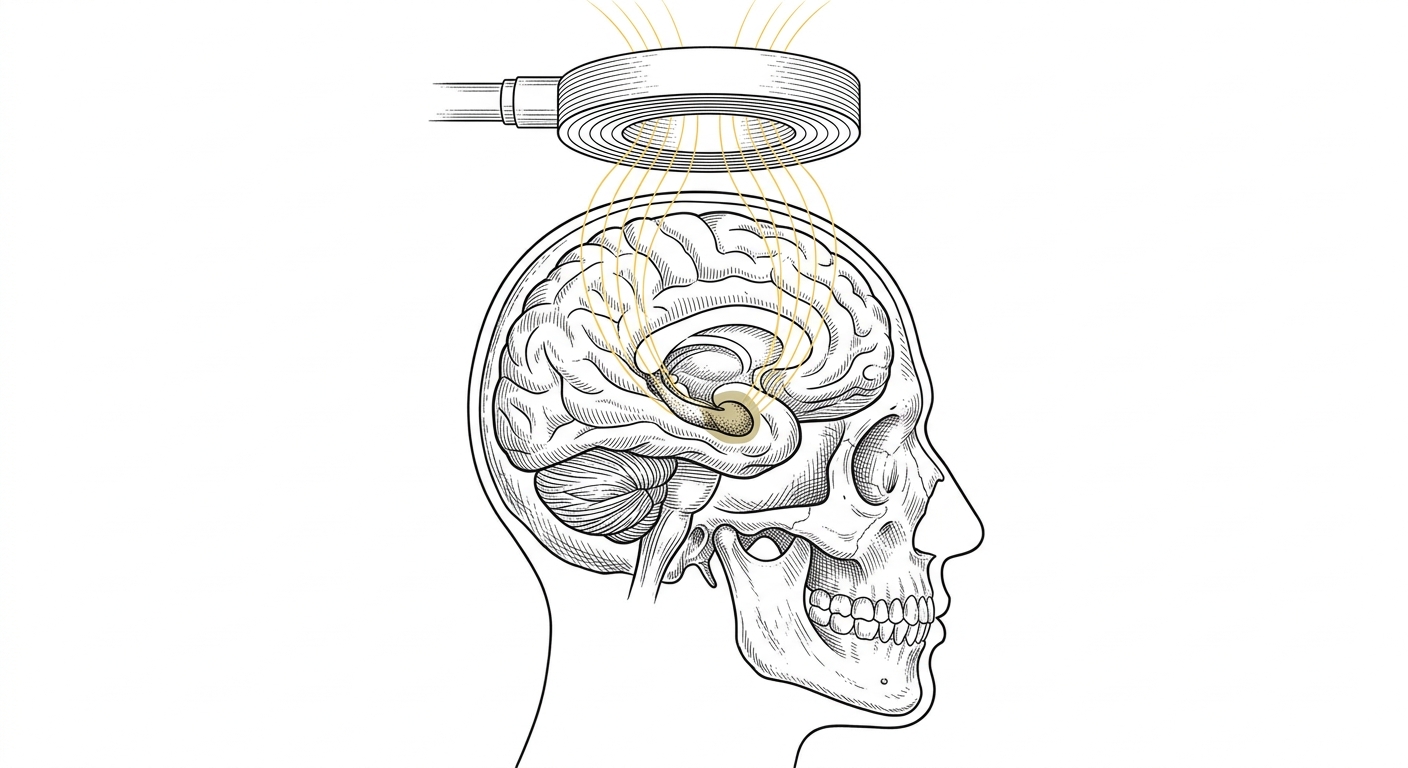
The effort, called the PREVENT Study, received $1,229,954 from the National Institute of Mental Health. It centers on a technology called transcranial magnetic stimulation, or TMS, which uses magnetic pulses to influence brain activity from outside the skull. TMS has been FDA-cleared for treatment-resistant depression since 2008, but using it as a *preventive* intervention in the immediate aftermath of trauma is a new frontier.
The scientific case rests on roughly a decade of research showing that people with an overactive amygdala, the brain's threat-response center, in the first week after trauma are significantly more likely to go on to develop chronic PTSD. The Emory team's hypothesis: dampen that early hyperreactivity with targeted TMS, and you may be able to interrupt the cascade of symptoms before it becomes a lasting disorder.
Participants will be recruited from Grady Memorial Hospital, Atlanta's public safety-net hospital and one of the largest in the Southeast. Grady sees high volumes of trauma patients, including survivors of violent crime, gunshot wounds, and serious accidents, and serves a predominantly low-income, Black population that bears a disproportionate share of Atlanta's trauma burden. Emory's longstanding Grady Trauma Project gives researchers an established recruitment infrastructure and community trust in a population often underrepresented in neuroimaging research.
The study runs in two phases. In the first, researchers will verify that TMS actually reduces amygdala reactivity in trauma survivors and establish the right dosage, while monitoring closely for safety. Only if those benchmarks are met will the team proceed to a full randomized controlled trial tracking PTSD and depression symptoms over three months. The phased design reflects the field's hard-learned caution: earlier attempts at post-trauma prevention, including widely used psychological debriefing protocols, were later found to be ineffective or even harmful.
The need for prevention tools is stark. About 70% of Americans will experience at least one traumatic event in their lifetime, yet emergency departments, which see millions of trauma survivors every year, have almost no clinical infrastructure for intervening in the window between trauma exposure and disorder onset. Roughly 6% of Americans will develop PTSD, with rates far higher among combat veterans, assault survivors, and communities with sustained exposure to violence. In Georgia, where mental health providers are scarce across much of the state and many low-income residents lack coverage for mental health follow-up care, a scalable prevention approach could carry particular weight.
If the trial's safety and target-engagement milestones are met, the study will advance to a double-blind randomized trial, with full results expected within a few years.